Laparoscopy and dye test
The laparoscopy and dye test is widely considered to be the golden standard method to check the Fallopian tubes, particularly in high-risk patients (women with a past history of pelvic infection, appendicitis, chlamydia, pelvic and abdominal surgery, tubal surgery, ectopic pregnancy). Laparoscopy is a minimally invasive procedure in which a fibre optic telescope called laparoscope is inserted through a small cut under the belly button. Laparoscopy allows the internal organs of the abdomen and pelvis to be inspected visually and excludes other problems such as endometriosis, fibroids, ovarian cysts and adhesions (scar tissues). Most infertile couples require a diagnostic laparoscopy for complete evaluation of their infertility. Among women whose tubes were found to be unobstructed using HSG, 18% were found to have tubal obstruction or peritubal adhesions using laparoscopy and a further 34% were found to have endometriosis or fibroids.
The laparoscopy procedure is usually done as a day case surgery under general anesthetic. It takes about 15-30 minutes.
When performing the laparoscopy procedure, a fine needle is inserted into the abdomen and gas (carbon dioxide) is pumped into the abdomen to push the intestine away. A fibre-optic telescope (laparoscope) is then inserted through a small incision under the belly button; (this leaves a minute scar which is almost invisible). A powerful light is then shone down through the laparoscope. The doctor then inspects the inside of the abdomen and pelvis including the outside of the womb, the tubes and ovaries. A second incision might also be made so that a probe can be inserted in order to move pelvic organs such as the ovaries into clear view.
A colored dye (methylene blue) is then injected through the cervix. If the tubes are not blocked the dye should pass along them and spill into the abdomen.
Laparoscopy showing normal uterus, ovaries and fallopian tubes

Dye seen spilling from the Fallopian tube

Laparoscopy showing hydrosalpinx

Dye seen spilling from the Fallopian tube

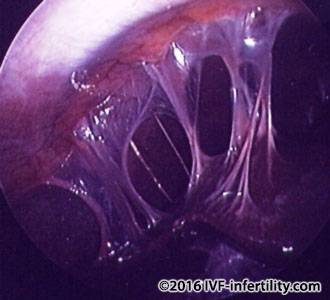
Laparoscopy showing pelvic adhesions

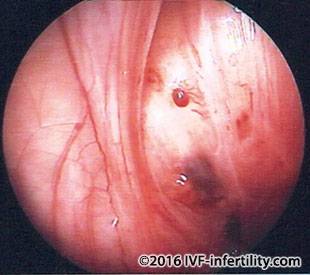
Laparoscopy showing perihepatic adhesions
Laparoscopy showing bicornuate uterus

Laparoscopy showing double uterus with one non functioning

Laparoscopy showing mild endometriosis
If an abnormality is found during laparoscopy, this may be dealt with at the same time thus avoiding another operation. When performing operative laparoscopy such as opening of blocked tubes, cutting of adhesions and freeing of the tubes etc. Additional instruments such as micro-scissors and forceps are placed in the abdomen through an additional cuts.
When the surgery is completed, the gas is removed and a stitch may be inserted to close the incision. After the laparoscopy procedure the patient may experience some discomfort and shoulder tip pain, this is due to the gas that was injected into the abdomen. She may also feel bloated. The discomfort usually lasts about 24-48 hours.
Diagnostic laparoscopy is associated with a proximately 3% risk of minor complications such as nausea and shoulder tip pain. The risk of major complications such as bowel injury, ureteric and bladder injury and injury to blood vessel is about 0.6-2 /1000. (Chaperon et al. Human Reproduction 1998; Harkki-Siren et al. Obstet Gynecol.1999)