Ovulation tests
Women with normal (regular) menstrual cycles are likely to be ovulating. It is important to remember that every woman may fail to ovulate from time to time, so a single negative ovulation test is meaningless. The main methods for detecting ovulation are detailed below.
Basal body temperature chart (BBT)
This is a simple but unreliable method to detect ovulation. The idea behind the ovulation test is that in women who are ovulating normally, the body temperature drops immediately before ovulation and rises 0.5 - 1.0°c after ovulation, which is maintained for the remainder of the cycle. The temperature then falls back before the menstrual flow begins. The temperature rise is caused by the progesterone secretion from the corpus luteum after ovulation. BBT allows the patient to determine for her self if she is ovulating and the approximate time of ovulation in retrospect.
Commercially available ovulation detection kits (urine dip-stick)
This is a simple test and involves dipping a chemically treated strip e.g. “clearplan” or “ovu Quick” into the urine and assessing the color changes which measure Luteinizing hormone (LH). The idea is to detect when the levels of the hormone, LH starts to rise. Ovulation usually occurs about 36 hours after the start of the rise of LH. Thus allowing intercourse to be timed at the most fertile period.
Blood progesterone
This is the gold standard test; it is a simple blood test to measure the levels of the hormone progesterone. Progesterone levels start to rise a few hours before ovulation and peaks about 7 days after ovulation. It then starts to drop, unless the woman is pregnant. A high level (>30 nmol/l ) is a good retrospective evidence that ovulation occured. The test is not 100% reliable. The ovary may produce large amounts of progesterone without releasing the egg (this is called luteinized unruptured follicle), or ovulation may take place without a marked rise in the progesterone level (called luteal phase defect).
Ultrasound scans
Serial ultrasound scanning can detect the development of the follicle (a thin-walled structure containing fluid with an attached egg to its wall) and its collapse after ovulation. Vaginal ultrasound scan is not only much more comfortable to the patient but it also gives a much clearer picture than the abdominal ultrasound scan. The follicle is usually ready for ovulation when it measures 1.8 - 2.5 cm in diameter.

Endometrial biopsy
This is not a very reliable method of detecting ovulation. The ovulation test involves taking a small strip from the lining of the womb (endometrium). The strip is then stained and examined under a microscope. The procedure is performed about a week before the expected period i.e. about 7 days after ovulation. The idea is that after ovulation, the hormone progesterone will induce secretary changes in the endometrium glands. It should be noted that the procedure may cause uterine cramps and discomfort and there is a very small risk that an early pregnancy could be disrupted.
Tests to find out the cause of non ovulation
Blood prolactin level
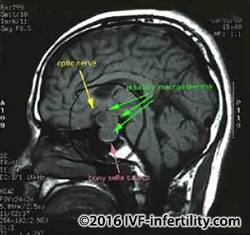
This is a simple blood test to measure the blood level of prolactin; the idea is that too much of prolactin (milk hormone) may prevent ovulation. If the prolactin level is elevated, the test needs to be repeated to confirm that it is a persistent problem. Prolactin levels could be raised due to stress. If prolactin levels are persistently high, MRI of the pituitary gland is recommended to exclude prolactinoma.
FSH, LH, Estradiol and free Androgen blood levels
Measurements of these hormones needs to be carried out at a particular time during the woman's menstrual cycle (usually between day 2-4 of menstruation) for the results to be valid. High FSH level combined with low Estradiol level indicates primary ovarian failure while low FSH levels and low Estradiol levels may indicate disorders of the pituitary or hypothalamus glands. Normal FSH, normal Estradiol level and high LH may indicate PCOS.
Anti-Mullerian hormone (AMH)
This hormone is produced by the ovaries (from the granulosa cells of pre-antral follicles) and hence serum AMH levels correlate with follicle pool. AMH levels decline sharply with advancing maternal age, they are not influenced by cycle day so can be performed any day of the cycle. The result is not affected by previous hormone treatment such as contraceptive pills. Furthermore, there are minor inter-cycle variabilities compared with FSH, LH and Estradiol. AMH levels appear to be the best hormonal test for ovarian reserve. AMH levels can predict poor and over responders and thus allows optimal stimulation protocol for IVF treatment. A level of less than or equal to 5.0 pmol/l usually indicate a low response while a level greater than or equal to 40.0 pmol/l will indicate high response. A recent study found women with high AMH levels were 2.5 times more likely to have a successful IVF cycle than women of a similar age with low levels of the hormone. The researcher commented that AMH levels were a predictor of pregnancy and live birth, even when the mother's age and egg production were taken into account (JCEM, 2013). It appears that although AMH level is a good predictor of ovarian response, AMH levels are not good predictor for pregnancy outcomes in IVF in young women. Furthermore, pregnancies were reported in women with undetectable AMH levels.